Key Takeaways
- The tarsal plate helps each eyelid keep its shape, position, and stability during blinking.
- The upper tarsal plate contains meibomian glands that release oil into the tear film and help reduce tear evaporation.
- Related structures such as the superior transverse ligament, medial palpebral ligament, and facial arteries help support eyelid movement, position, and blood supply.
- Tarsal plate damage can affect eyelid alignment, tear distribution, eye comfort, and the need for surgical repair.
What Is the Tarsal Plate?
The tarsal plate is a firm plate of tissue inside the eyelid. It sits near the eyelid margin and helps the lid keep its shape during blinking, opening, and closure. Each eyelid has a tarsal plate, with one in the upper lid and one in the lower lid.
When people ask what is the tarsal plate of the eyelid, the simplest answer is that it acts as the internal framework of the lid It is not bone or cartilage, even though it has a firm feel.
It is made mainly of dense connective tissue, which gives it strength while still allowing normal movement.
The tarsal plate also helps protect the eye surface. It supports lid alignment so blinking can spread moisture across the cornea. This helps maintain a stable tear film and reduces friction between the eyelid and eye.
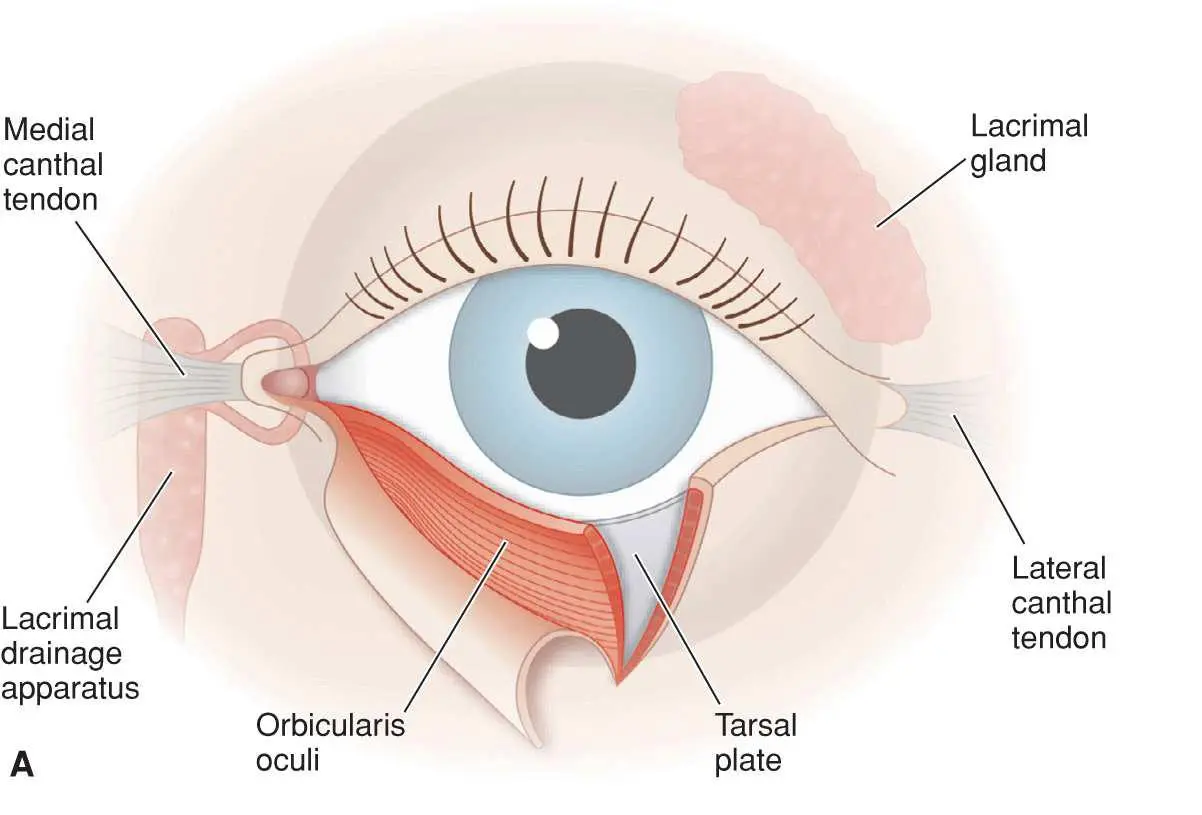
Tarsal Plate Anatomy
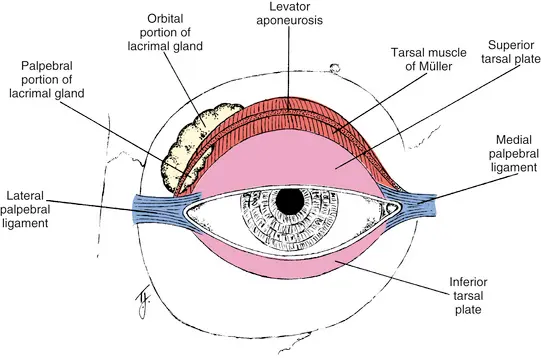
Tarsal plate anatomy includes the upper and lower tarsal plates, their connective tissue, glandular structures, and nearby attachments. The upper plate is larger and more curved. The lower plate is smaller but still important for lower lid stability.
The tarsal plates sit close to the inner surface of the eyelids. This inner layer is lined by the palpebral conjunctiva, a smooth membrane that faces the eye.
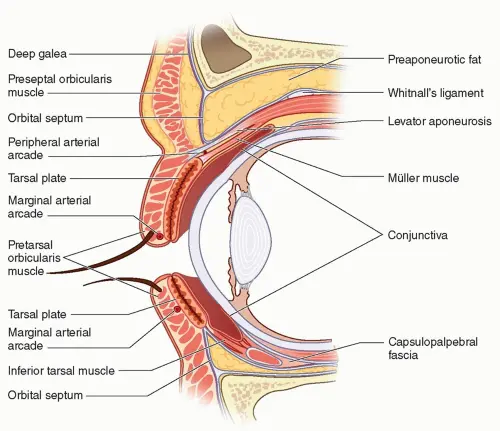
A sagittal section of the eyelid shows how the tarsal plate sits between the outer skin and the inner conjunctival surface.
Important parts of tarsal anatomy include:
- Dense connective tissue that gives the eyelid support.
- Meibomian glands that help protect the tear layer.
- The palpebral conjunctiva that lines the inner eyelid.
- Attachments that connect the lid to nearby orbital structures.
Tarsal Plate Eyelid Histology
Tarsal plate eyelid histology refers to the tissue makeup of the plate under microscopic review. The main structural material is dense connective tissue. This tissue has tightly arranged fibers that resist stretching and help preserve eyelid shape.
Loose connective tissue sits in nearby eyelid layers. It allows tissue planes to move and shift during facial expression, blinking, and surgery. The difference between dense and loose tissue matters because each layer behaves differently.
The tarsal plate also contains glandular structures. These glands release oil that supports the tear layer. When they become blocked or inflamed, the eyelid margin may feel tender, irritated, swollen, or form eyelid bumps
Superior and Inferior Tarsal Plates
The superior tarsal plate sits inside the upper eyelid. It is larger than the lower plate and helps maintain the upper lid curve. The superior tarsus is often wider in the center and narrower toward the sides.
The inferior tarsus sits inside the lower eyelid. It has less vertical height than the upper plate, but it helps keep the lower lid close to the eye. The inferior tarsal plate also supports smooth lower lid movement during blinking.
The upper and lower plates differ because the lids have different jobs. The upper lid must lift, fold, and close over more of the eye. The lower lid moves less, but it must remain stable against gravity and facial motion.
What the Upper Tarsal Plates Contain
The tarsal plates of the upper eyelid contain meibomian glands, which are oil-producing glands located within the tarsal tissue. These glands open near the eyelid margin and release oil into the tear layer. This oil helps slow tear evaporation.
Meibomian glands are modified sebaceous glands. In regular skin, sebaceous glands produce oil for the skin and hair. In the eyelid, these glands support the ocular surface instead.
The upper eyelid usually contains more meibomian glands than the lower eyelid. Their openings sit near the lid margin, where the oil layer can enter the tears. This explains why eyelid inflammation and dry eye symptoms often overlap.
Tarsal Plate Function
Tarsal plate function begins with support. The plate gives the eyelid enough firmness to protect the eye and enough flexibility to move with each blink. Without this support, the lid could lose shape or fail to rest correctly against the eye.
The tarsal plate also works with muscles and ligaments. The orbicularis oculi muscle closes the eyelids, while upper lid retractors help lift the upper lid. The tarsal plate provides a stable base for these movements.
Its main functions include:
- Supporting eyelid shape and lid margin position.
- Helping blinking spread tears evenly.
- Supporting meibomian gland oil delivery.
- Protecting the cornea from exposure and irritation.
Eyelid Shape and Support
The tarsal plate helps define the shape of the eyelid. It gives the lid a stable edge and supports the eyelid margin. This alignment matters because the margin must rest close to the eye without turning inward or outward.
The plate also helps the lid resist distortion. Aging, trauma, inflammation, and surgery can affect eyelid tissues. A firm internal structure helps the lid maintain better position during these changes.
The upper plate also contributes to upper eyelid contour. Its relationship with surrounding skin, fat, muscle, and connective tissue affects how the upper lid sits. The tarsal plate does not control the eyelid alone, but it plays an important support role.
Tear Film Stability
The tear film is the thin moisture layer that covers the eye surface. It keeps the cornea smooth, clear, and comfortable. The tarsal plate supports tear film stability by helping the lid margin stay aligned.
The meibomian glands inside the tarsal plate add oil to the tear layer. This oil reduces evaporation and helps tears stay on the eye longer. When the oil layer is poor, the eye may burn, sting, or feel gritty.
Lid position also affects tear spread. If the lid margin does not meet the eye evenly, tears may not distribute well. This can cause dry spots, reflex tearing, or fluctuating vision.
Meibomian Gland Function
Meibomian gland function is closely tied to the tarsal plate. These glands produce oil for the outer layer of the tear film. This oil helps reduce evaporation during reading, screen use, and daily visual tasks.
Blocked glands can change the quality or amount of oil reaching the lid margin. This may cause redness, irritation, crusting, or dry eye symptoms. A blocked gland may also form a chalazion, which is a firm eyelid bump caused by trapped gland material.
If the tarsal plate or eyelid margin becomes scarred, gland drainage may change. This can affect eye surface comfort over time. A complete eyelid exam often includes inspection of the lid margin and gland openings.
Tarsal Plate Attachment
Tarsal plate attachment refers to how the plate connects with nearby eyelid and orbital structures. These attachments help hold the eyelids in place. They also allow the lids to move while staying anchored at the inner and outer corners.
The tarsal plates connect to the orbit through ligaments and nearby connective tissue. The orbit is the bony socket around the eye, and the orbital rim forms the front border of that socket. Weakness, trauma, or scarring in these support structures can change lid position.
Attachments matter during eyelid surgery. During blepharoplasty, ptosis repair, or reconstruction, the surgeon must understand where the tarsus connects and how nearby layers move.
Dr. Kopelman’s clinical evaluation of eyelid anatomy includes the relationship between the tarsal plate, lid margin, and surrounding support tissues.
Medial Palpebral Ligament
The medial palpebral ligament supports the inner corner of the eyelids. It helps hold the tarsal plates in position near the nose. This ligament also sits close to the tear drainage system and the orbicularis oculi muscle.
If medial support weakens or shifts, the inner eyelid position can change. This may affect how the lid rests against the eye. It may also affect tear flow near the inner corner.
The medial attachment helps maintain the shape of the eyelid opening. If it is damaged by trauma, scarring, or surgery, repair may require careful reconstruction. The goal is to restore support and protect the eye surface.
Orbital Septum
The orbital septum is a connective tissue layer that separates eyelid tissue from deeper orbital contents. It attaches near the orbital rim and relates closely to the tarsal plate and lid retractors. In the upper eyelid, it sits near the levator system and preaponeurotic fat.
The septum is not the same as the tarsal plate. The tarsal plate gives firmness to the lid margin, while the septum helps organize deeper eyelid tissues. Both structures matter because they interact within the layered anatomy of the eyelid.
The orbital septum can affect eyelid fullness. Fat behind the septum may become more visible with aging or tissue laxity. Skin, muscle, fat, ligaments, and the tarsal plate all contribute to eyelid contour.
Related Eyelid Structures
The tarsal plate works with several nearby structures that help the eyelid blink, protect the eye, and stay properly aligned. These structures include:
- Palpebral conjunctiva: Lines the inner surface of the eyelid.
- Eyelid margin: Supports tear spread, lash position, and gland openings.
- Orbicularis oculi muscle: Helps close the eyelids during blinking.
- Superior tarsal muscle: Helps support upper eyelid elevation.
- Medial palpebral ligament: Anchors the inner eyelid corner.
- Orbital septum: Separates eyelid tissue from deeper orbital contents.
Together, these layers explain why eyelid symptoms can have more than one cause. Dryness may involve gland function, tear quality, or lid position. Drooping may involve muscle, tendon, nerve input, or tarsal support.
Palpebral Conjunctiva
The palpebral conjunctiva lines the inner surface of the eyelids. It lies against the inner side of the tarsal plate and faces the eye surface. This smooth membrane helps the eyelid glide over the eye during blinking.
The palpebral conjunctiva differs from the bulbar conjunctiva. The bulbar conjunctiva covers the white part of the eye. These two conjunctival areas work together to allow comfortable movement between the lid and eye.
Because the conjunctiva sits close to the tarsal plate, inflammation or scarring can affect eyelid movement. Inner eyelid irritation may cause burning, redness, or a foreign body sensation. Persistent symptoms should be evaluated.
Eyelid Margin
The eyelid margin is the edge of the eyelid where lashes, gland openings, and the tear film interface meet. It must stay smooth and aligned to protect the eye. The tarsal plate supports this edge from within.
The meibomian gland openings sit along the margin. Oil from these glands enters the tear layer at this point. If the openings become blocked, the margin may look red, thickened, or irregular.
The lid margin also matters in surgery and repair. Small changes can affect lash direction, tear spread, and corneal comfort. A stable margin helps reduce rubbing, exposure, and irritation.
Orbicularis Oculi Muscle
The orbicularis oculi muscle is the circular muscle that closes the eyelids. It allows gentle blinking and tighter eyelid closure. Its movement helps spread tears and protect the eye.
This muscle works with the tarsal plate and eyelid ligaments. Some fibers support routine blinking, while others help with forceful closure. The muscle also relates to the tear pump near the inner corner of the eyelids.
Weakness of this muscle can cause incomplete eyelid closure. This may happen with facial nerve problems or injury. If the eye cannot close fully, dryness or exposure may occur.
Superior Tarsal Muscle
The superior tarsal muscle is a small smooth muscle in the upper eyelid. It helps support upper eyelid elevation along with the levator system. This muscle is also called Müller’s muscle.
Some searches use the phrase superior tarsal muscles, but eyelid anatomy usually refers to the superior tarsal muscle. It attaches near the upper tarsal region and has sympathetic nerve input. Changes in its function can affect lid height.
The tarsal muscle matters in ptosis evaluation. If the upper lid sits too low, clinicians assess muscle function, tendon position, nerve input, and tarsal support. A complete exam helps identify the main cause.
What Happens if It Is Damaged?
Damage to the tarsal plate can affect eyelid position, lid stability, and eye surface protection. Damage may result from trauma, prior surgery, scarring, tumors, burns, or inflammation. The effect depends on the size, depth, and location of the injury.
Common effects may include:
- Eyelid drooping or notching.
- Lid turning inward or outward.
- Dryness, tearing, or irritation.
- Poor lid closure.
- Changes in meibomian gland drainage.
- Corneal exposure or rubbing.
The tarsal plate helps keep the lid margin stable. If it weakens or becomes distorted, the eyelid may not sit correctly against the eye. This can cause redness, foreign body sensation, or blurred vision.
Eyelid Position Changes
Eyelid position changes can include drooping, retraction, inward turning, outward turning, or margin notching. These changes affect both appearance and function. The main concern is whether the eyelid still protects the eye surface.
Upper eyelid changes may affect vision if the lid blocks the pupil. Lower eyelid changes may cause tearing or exposure if the lid pulls away from the eye. A distorted margin may cause lashes to rub the cornea.
Evaluation often includes lid height, closure, margin position, tear quality, and eye surface findings. The clinician may also look for scarring, laxity, or tissue loss. These findings help guide treatment.
Tear Film Problems
Tear film problems can occur when eyelid structure changes. The eyelids spread tears across the eye with each blink. If the lid margin does not contact the eye evenly, the tear layer may break up faster.
Meibomian gland dysfunction can also affect tear quality. The oil layer may become too thin or irregular. Without enough oil, tears evaporate more quickly.
Some tear problems improve with lid hygiene, lubrication, and treatment of inflammation. Others need structural correction if lid position is the main cause. The correct approach depends on the diagnosis.
When Repair May Be Needed
Repair may be needed when the eyelid cannot protect the eye, maintain position, or support the lid margin. This may happen after trauma, tumor removal, severe scarring, or complications from earlier surgery. The need for repair depends on function, not only appearance.
Tarsal repair may involve tightening, repositioning, grafting, or reconstruction. The method depends on how much tissue is missing and which layers are affected. Surgeons may need to restore the plate, margin, conjunctiva, skin, and muscle balance.
Recovery depends on the type of repair. Swelling, bruising, temporary tightness, dryness, or irritation may occur. Risks can include bleeding, infection, scarring, asymmetry, lid malposition, dry eye, or revision surgery.
Why It Matters in Eyelid Surgery
The tarsal plate matters in eyelid surgery because it helps define lid shape, support, and function. Procedures near the eyelid must preserve or restore this support when possible. If the plate or its attachments are not respected, the eyelid can shift, become unstable, or fail to protect the eye surface properly.
The tarsal plate is especially important in procedures such as:
- Blepharoplasty: Helps maintain eyelid support and lid margin alignment.
- Ptosis repair: Assists with upper eyelid positioning and elevation.
- Eyelid reconstruction: Provides structural support after trauma, tumor removal, or tissue loss.
Eyelid surgery involves more than skin or fat removal. The surgeon must understand how the tarsus, muscles, ligaments, conjunctiva, and surrounding tissues interact during blinking and eyelid movement.
Dr. Kopelman’s background as a facial plastic and oculoplastic surgeon is relevant because these procedures require both structural and functional understanding of eyelid anatomy.
Blepharoplasty Planning
Blepharoplasty planning includes evaluation of eyelid skin, fat, muscle tone, lid position, and eye surface health. The tarsal plate helps the surgeon understand where support exists and how the lid margin should remain aligned.
Upper blepharoplasty may involve tissue near the levator system and superior tarsal plate.
The plate is not always directly altered during routine blepharoplasty. Still, its position and support influence planning. A patient with lid laxity, dry eye, or prior surgery may need a different approach than someone with stable lid anatomy.
Recovery may involve swelling, bruising, temporary dryness, and mild tightness. These symptoms can vary based on anatomy, surgical extent, and healing response. Patients should understand that eyelid healing is individual.
Ptosis Repair
Ptosis repair addresses a drooping upper eyelid. The cause may involve the levator muscle, levator aponeurosis, superior tarsal muscle, nerve input, or tissue change. The superior tarsal plate can be relevant in surgical planning.
Ptosis can affect vision when the upper lid blocks the pupil. It may also cause brow strain because patients lift the eyebrows to see better. Evaluation may include lid height, crease position, levator function, and response to testing.
Ptosis repair has limits and risks. Possible issues include undercorrection, overcorrection, asymmetry, dry eye symptoms, contour irregularity, or need for revision. A direct exam is needed to assess candidacy.
Eyelid Reconstruction
Eyelid reconstruction may be needed after trauma, tumor removal, burns, scarring, or tissue loss. The tarsal plate becomes important because the eyelid needs internal support to protect the eye. Reconstruction often requires attention to both the anterior and posterior eyelid layers.
The posterior layer includes the tarsus and conjunctiva. The anterior layer includes skin and muscle. A stable reconstruction should allow blinking, protect the cornea, and maintain a smooth margin.
Reconstruction carries risks because the eyelid is small and complex. Scarring, lid notching, irritation, asymmetry, or exposure can occur. Some patients may need more than one procedure.
When to See an Eyelid Specialist
You should consider an eyelid specialist when symptoms affect comfort, vision, or eye protection.
Warning signs include persistent drooping, inward or outward turning, incomplete closure, chronic tearing, repeated chalazia, or irritation that does not improve. A new eyelid lump, bleeding lesion, or non-healing area also needs medical evaluation.
An eyelid specialist can assess the tarsal plate, lid margin, conjunctiva, tear film, and nearby support structures.
The exam may include lid measurements, eye surface review, and inspection of meibomian gland openings. In some cases, imaging or biopsy may be needed.
This article explains anatomy and general surgical relevance, but it does not replace a diagnosis. Eyelid conditions vary by cause, severity, age, eye surface health, and prior procedures.
A medical evaluation helps connect symptoms with the correct anatomical source.